

Confirmation of a serious illness, recurrence of disease, unexpected clinical findings, complex co-morbidities, and even a terminal prognosis, are all examples of difficult information that must be communicated by physicians.
A recent Health Affairs Blog post by health services researcher Vincent Mor, Ph.D., of Brown University in Providence, RI, noted physicians’ reluctance to have conversations about prognosis or advance care planning.
While they acknowledged the importance of such conversations, nearly half were frequently unsure of what to say.
Medical News Today asked practitioners from the field of palliative care, who deal with situations wherein patients face serious or life-threatening illnesses on a daily basis, to share their experience.
“This is not easy. Nobody likes doing it. No matter how well you deliver bad news, it’s still bad,” said Steven Pantilat, M.D., founding director of the Palliative Care Program at the University of California-San Francisco Medical Center. “You can’t make it somehow O.K. for the patient, but it’s important not to make it worse.”
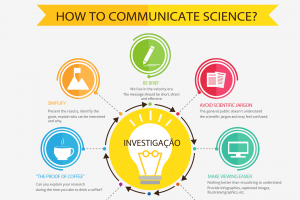
Find out which strategies work for experienced practitioners when they talk to patients and their families about serious medical issues.
Clear communication is key
When bad news hits, patients are faced with difficult choices. They have to consider trade-offs between cure-focused and comfort-oriented care to make personal values-based decisions about their own treatment.
Most people would want to know the truth – no matter how upsetting it proves to be. It is also important to arm them with this information to allow them to make informed decisions about their care.
Dr. Pantilat illustrated the challenge with a patient of his who was 89 years old but still driving and an active ballroom dancer. One day, he came to the emergency room complaining of hip pain. An X-ray and computerized tomography scans showed two masses of untreatable colon cancer, totally unsuspected.
“And now I have to tell him this terrible news,” he explained to MNT. “I told him in simple language, and then I was just quiet. We as physicians don’t always appreciate just how bad the news will be to someone who still thinks their tomorrows are infinite.”
Dr. Pantilat recently published a book entitled Life After the Diagnosis: Expert Advice on Living Well with Serious Illness for Patients and Caregivers, which encapsulates 27 years of medical practice in helping patients to live well in the face of serious illnesses.
Although the book was written for lay people, the information can also help clinicians to understand their patients’ experiences and learn to talk with them about shocking news.
He recommended delivering bad news clearly and straightforwardly. “Don’t use jargon or euphemisms. It is what it is, and it has a name. Then give the patient some time to respond.”
Sometimes doctors are so uncomfortable that they just keep talking in order to avoid drawn-out silences. Often, the patient doesn’t absorb much after the first shock of the bad news hits. In some cases, it may be preferable to save planning and follow-up questions for a subsequent meeting, after their shock has dissipated.
It’s O.K. to say ‘I’m sorry’
“Don’t ask: ‘Do you have any questions?’ because the answer will often be no. Instead ask: ‘What questions do you have?'” Dr. Pantilat advised.
Acknowledge the patient’s feelings. “But don’t say, ‘I know how you’re feeling,’ or ‘The same thing happened to one of my own family members.'”
Such attempts to personalize the situation are not helpful, but you can show empathy: “I can see how devastating this news is for you. It must come as a big shock.”
It also helps for the clinician to prepare in advance the care plan that he or she would recommend, Dr. Pantilat noted. Patients may come to these meetings already on edge. “People know that good news doesn’t wait. Bad news is what follows when the doctor says: ‘Why don’t you come into my office and have a seat?'”
It may help to let patients know when a diagnostic test is first ordered that an unwanted outcome is a real possibility, even if the goal for the test is to rule it out.
It’s O.K. for doctors to say how sorry they feel – even though the doctor is not to blame.
He also advised ensuring that the patient knows they won’t be abandoned, but that the physician will continue to accompany them throughout their treatment.
How best to facilitate family meetings
How to better facilitate this kind of conversation is a skill that can be learned, Timothy Jessick, Doctor of Osteopathic Medicine (D.O.), a palliative care physician at Aurora West Allis Medical Center in Wisconsin, told MNT.
He has developed a 4-hour training program that draws on professional resources from the Palliative Care Network of Wisconsin to teach hospitalist physicians communications skills that enable them to lead goals-of-care conversations with critically ill, hospitalized patients.
This intervention is designed for hospitalized patients who may have 12 months or under to live.
“What we’re trying to do is help hospitalists change their mindsets to be more person – and patient-centered – to meet the family where they are at and to help them define goals of care and treatments that make sense for them now,” Dr. Jessick said.
More than 150 Aurora doctors and nurses have received this training in how to lead goals-of-care conversations, and there are plans to train 100 more hospitalists and 130 emergency clinicians throughout the Aurora health system over the next 18 months.
“We believe our hospitalists can and should be doing more than just episodic care for this hospitalization. That includes helping to establish goals of care that can be documented in the patient’s medical record and accompany the patient across care settings,” Dr. Jessick added.
Still, the moment of truth will come when bad news has to be delivered. Dr. Jessick remembers vividly how difficult that was for him to do for the first time, even though it was 20 years ago.
“There was no one available with the knowledge or expertise to help me with this most difficult conversation,” he recounted.
He recommended being well prepared for the meeting. Physicians should ask the patient and their family if this is the right time to share important information, or if other family members need to be present.
Asking open-ended questions and finding out what the patient has already been told, as well as what they understand about their condition, is also important.
Adding the human touch
For Frank Ostaseski, co-founder of San Francisco’s Zen Hospice Project and director of the Metta Institute in Sausalito, CA – which was established in 2004 to provide Buddhist-inspired education on spirituality to health professionals through the End-of-Life Practitioner Program – the challenge of communicating bad news requires more than a good script and an intention to be compassionate.
“It’s also about the professional’s own humanity and self-awareness. This is what cultivates the resilience needed to care profoundly without becoming overwhelmed and to sustain this work for the long haul without burnout,” he explained to MNT.
Ostaseski’s new book, The Five Invitations: Discovering What Death Can Teach Us About Living Fully, distills 30 years of his bedside experience with more than 2,000 patients and the training of countless healthcare professionals in mindfulness meditation and compassionate approaches to care. It supports professionals in addressing the ultimate in bad news: a terminal diagnosis.
In difficult conversations about bad news, patients particularly crave a human face from their healthcare provider, Ostaseski said. But according to him, doctors are not taught to listen with full attention and without interference.
“Self-awareness is required for empathetic attunement, and ultimately leads to a more compassionate connection with patients,” he explained.
“Mindfulness training is not new-age gobbledegook. There are more than 3,000 well documented studies on its efficacy. Mindfulness is predominantly about paying attention, on purpose, to what matters most, and bringing your whole self to the experience,” Ostaseski added.
Using simple language, listening to the patient, showing empathy, and having clear suggestions for the patient’s care management plan, are all strategies that experienced practitioners have employed when discussing bad news with patients.
Empathy and clear communication are at the heart of patient care, particularly when it comes to addressing difficult topics.
Source: Medical News Today
“It is the job of the clinician to help the patient redefine hope. If the hope was that the cancer would be cured, and if that is no longer possible, what can the patient hope for?”
Note: The UAlg Medicine Students have formation (through workshops) to deal with difficult situations and learn how to communicate with the patients.








{kind=link}